
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 




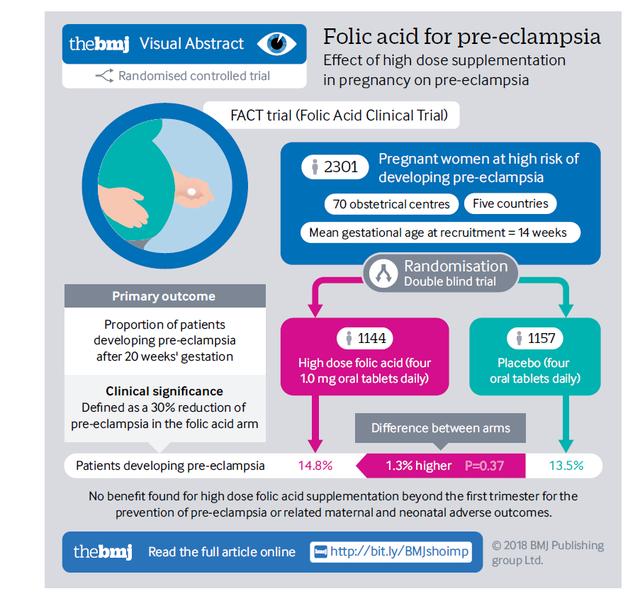

Preeclampsia, a condition unique to pregnancy, affects 5-10% of expecting mothers and is a significant threat to both maternal and fetal health, being a leading cause of maternal and perinatal mortality. Recent studies have revealed a strong correlation between homocysteine (HCY) levels in early pregnancy and the risk of developing preeclampsia.

The Link Between Early Pregnancy HCY and Preeclampsia
Researchers from Shanghai Jiao Tong University have identified a significant association between elevated homocysteine levels in early pregnancy and the risk of severe preeclampsia.
The retrospective cohort study included 147 cases of preeclampsia (103 mild and 44 severe) and 147 cases of gestational hypertension, with a control group of 4418 women who maintained normal blood pressure and proteinuria-free status throughout their pregnancies. Serum levels of homocysteine, folate, and vitamin B12 were measured from blood samples taken between the 11th and 13th week of gestation, and a logistic regression model was used to calculate adjusted odds ratios (aORs) and 95% confidence intervals (CIs).
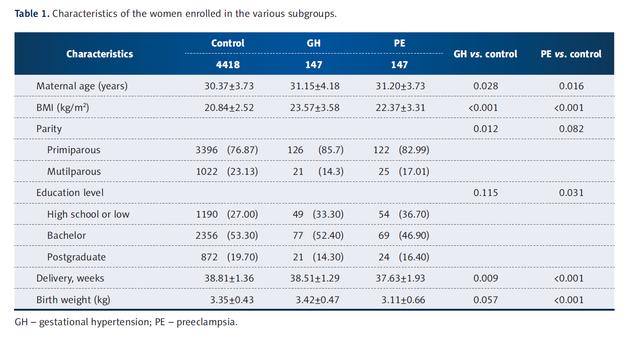
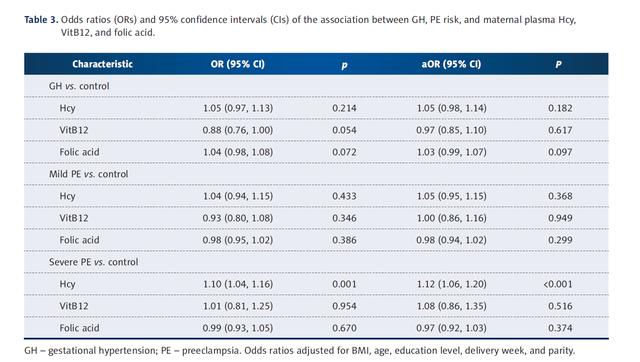
The study found that women who developed gestational hypertension and preeclampsia were older and had higher BMIs than the control group. Women with preeclampsia were less educated, while those with gestational hypertension were more likely to be first-time mothers. Notably, women with severe preeclampsia had significantly higher serum homocysteine levels than the control group (median: 8.50 μmol/L vs. 7.33 μmol/L, P<0.001). After adjusting for potential confounding factors, the adjusted odds ratio for homocysteine was 1.12 (95% CI 1.06–1.20).
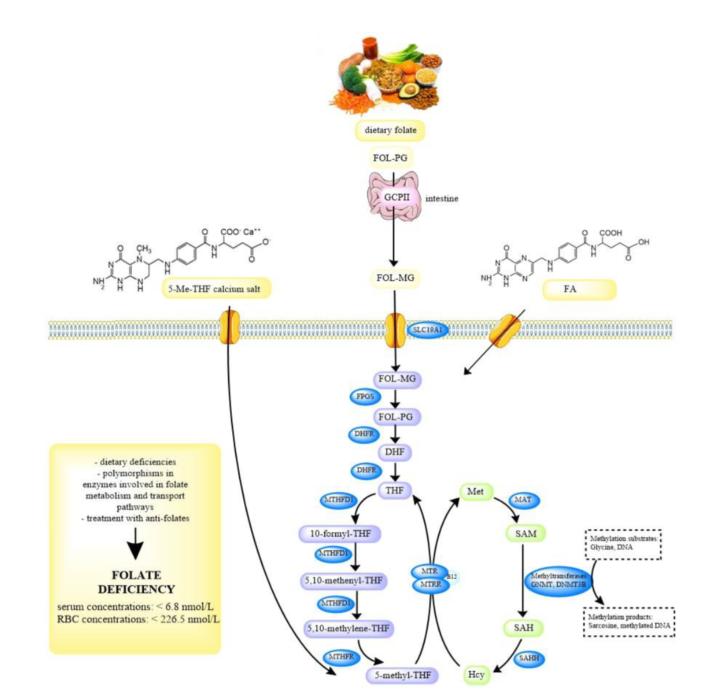
Homocysteine (HCY), a sulfur-containing amino acid, requires folate, vitamin B12, and the enzyme 5,10-methylenetetrahydrofolate reductase (MTHFR) for metabolism. Elevated HCY levels may contribute to preeclampsia by causing endothelial damage, promoting thrombosis, and inducing oxidative stress. Controlling HCY levels early in pregnancy can, therefore, be an effective strategy to reduce the risk of preeclampsia.
6S-5-Methyltetrahydrofolate: Reducing HCY Levels and Preventing Preeclampsia
6S-5-Methyltetrahydrofolate, the active form of folate, plays a crucial role in the metabolism of HCY. By donating a methyl group, it helps convert HCY back into methionine, thereby reducing HCY levels in the blood. Studies have shown that supplementing with 6S-5-methyltetrahydrofolate can improve folate metabolism, lower HCY levels, and decrease the risk of preeclampsia.
Among the various forms of 6S-5-methyltetrahydrofolate, Naturalization folate (Magnafolate) stands out for its high safety profile, which is particularly important for maternal and infant health. This form of folate is produced without the use of harmful substances like formaldehyde and p-toluenesulfonic acid, and it strictly controls the levels of impurities such as JK12A and 5-methyltetrahydrofolate calcium to non-toxic levels. It can rapidly increase serum and red blood cell folate levels, making it a preferred active folate for mothers and infants.

Reference
1. Sun, F., Qian, W., Zhang, C., Fan, J.-X., & Huang, H.-F. (2017). Correlation of Maternal Serum Homocysteine in the First Trimester with the Development of Gestational Hypertension and Preeclampsia. Medical Science Monitor, 23, 5396-5401. doi:10.12659/MSM.905055
2. Saccone G, Sarno L, Roman A, Donadono V, Maruotti GM, Martinelli P. 5-Methyl-tetrahydrofolate in prevention of recurrent preeclampsia. J Matern Fetal Neonatal Med. 2015; DOI: 10.3109/14767058.2015.1023189.
3. Lian Zenlin, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological characteristics and applications of folate and 5-methyltetrahydrofolate. Food Additives in China, 2022(2).
4. Lamers Y, Prinz-Langenohl R, Braumswig S, Pietrzik K. Red blood cell folate concentrations increase more after supplementation with [6S]-5-methyltetrahydrofolate than with folic acid in women of childbearing age. Am J Clin Nutr. 2006;84:156-161.


 Online Service
Online Service
