
 Español
Español Português
Português  русский
русский  Français
Français  日本語
日本語  Deutsch
Deutsch  tiếng Việt
tiếng Việt  Italiano
Italiano  Nederlands
Nederlands  ภาษาไทย
ภาษาไทย  Polski
Polski  한국어
한국어  Svenska
Svenska  magyar
magyar  Malay
Malay  বাংলা ভাষার
বাংলা ভাষার  Dansk
Dansk  Suomi
Suomi  हिन्दी
हिन्दी  Pilipino
Pilipino  Türkçe
Türkçe  Gaeilge
Gaeilge  العربية
العربية  Indonesia
Indonesia  Norsk
Norsk  تمل
تمل  český
český  ελληνικά
ελληνικά  український
український  Javanese
Javanese  فارسی
فارسی  தமிழ்
தமிழ்  తెలుగు
తెలుగు  नेपाली
नेपाली  Burmese
Burmese  български
български  ລາວ
ລາວ  Latine
Latine  Қазақша
Қазақша  Euskal
Euskal  Azərbaycan
Azərbaycan  Slovenský jazyk
Slovenský jazyk  Македонски
Македонски  Lietuvos
Lietuvos  Eesti Keel
Eesti Keel  Română
Română  Slovenski
Slovenski  मराठी
मराठी  Srpski језик
Srpski језик 




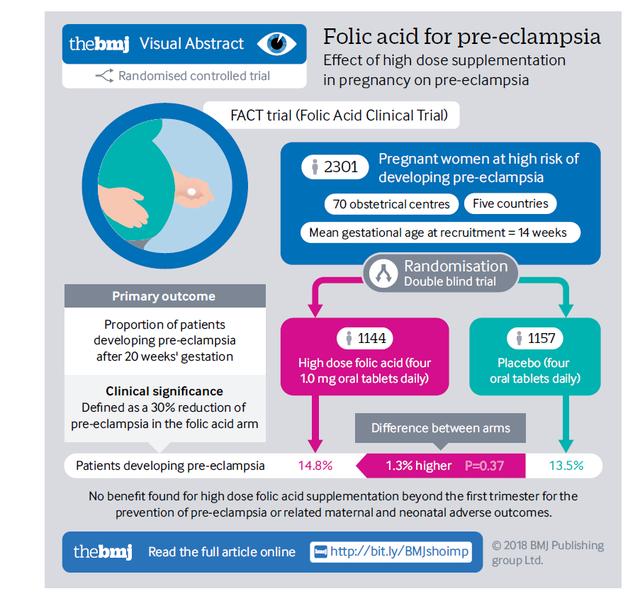

Is there a connection between Pregnancy-induced hypertension (Gestational hypertension), homocysteine (HCY) levels, and MTHFR?
Which type of folate should be supplemented during pregnancy?
The Relationship Between Gestational Hypertension and HCY Levels
A study published in 2021 revealed the association between gestational hypertension and homocysteine (HCY) levels in the blood.
The study included 360 pregnant women, with 180 in the observation group (gestational hypertension) and 180 in the control group (normal pregnancy), with an average age of 25.2±5.8 years. The data showed that the Hcy level in the observation group was 18.1±6.2 μmol/L, significantly higher than the 8.6±3.9 μmol/L in the control group (P<0.001). The HCY level in women with gestational hypertension was significantly higher than that in normal pregnant women.
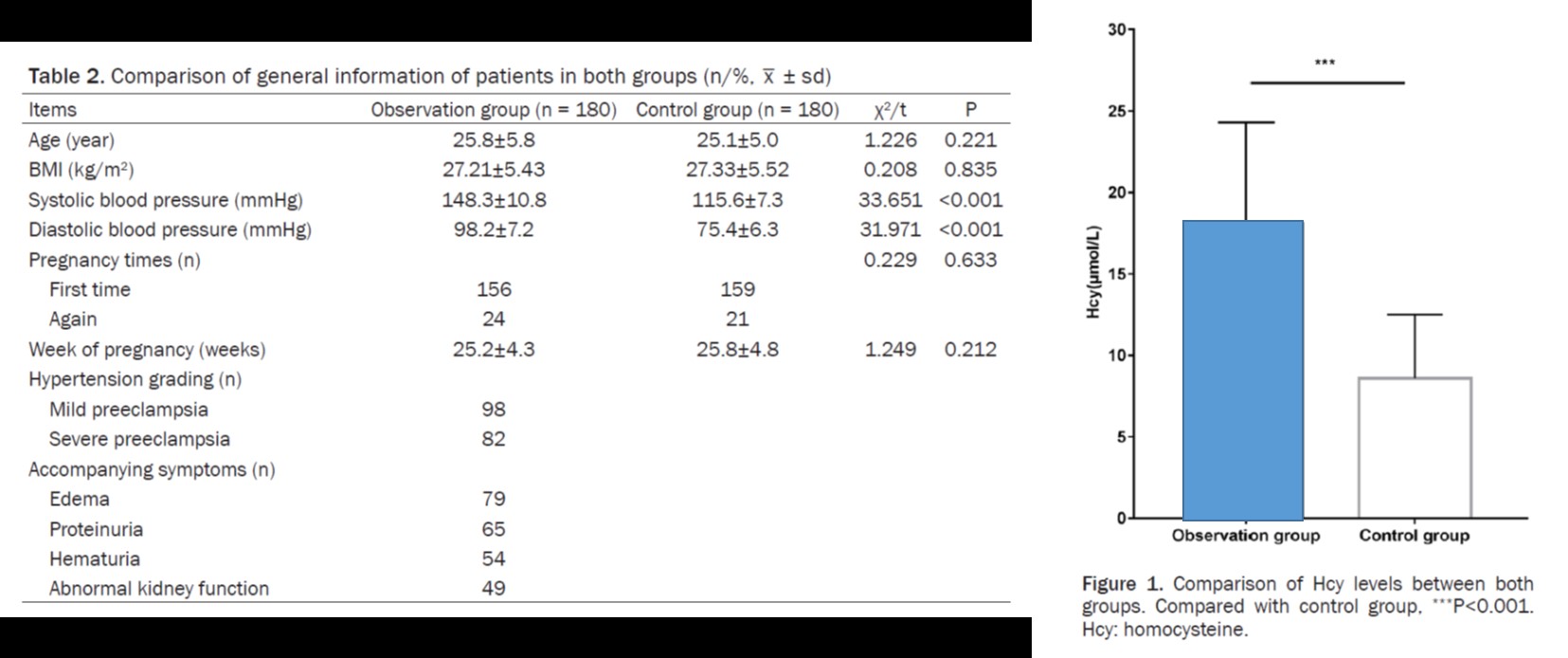
Further analysis of the data revealed that the proportion of women with the TT genotype was higher in the gestational hypertension group than in the control group, and women with the TT genotype had higher HCY levels and a higher incidence of adverse pregnancy outcomes.

Folate Supplementation and MTHFR Gene Polymorphisms: Naturalization Folate(Magnafolte)
MTHFR (5,10-methylenetetrahydrofolate reductase) plays a crucial role in folate metabolism. Polymorphisms in the MTHFR gene, particularly the C677T variant, can affect folate metabolism, leading to elevated HCY levels and increasing the risk of Pregnancy-induced hypertension (Gestational hypertension).
Therefore, choosing the appropriate folate supplement is particularly important for mothers with MTHFR gene variants.
For individuals with MTHFR-related folic acid metabolism, active folate (6S-5-methyltetrahydrofolate) is preferred due to its ability to bypass metabolic genes and be directly absorbed by the body.
Naturalization folate (Magnafolate) stands out as it is produced without harmful substances like formaldehyde and p-toluenesulfonic acid, and it strictly controls the levels of harmful impurities such as JK12A, 5-Methyltetrahydropteroic acid, achieving a non-toxic status.
Consequently, Magnafolate achieves a practically non-toxic level, can rapidly increase serum and red blood cell folate levels, and is a more suitable source of active folate for mother-to-be and infants.

References
1. Chinese Society of Cardiology, Women's Heart Health Study Group, & Chinese Society of Cardiology, Hypertension Study Group. (2020). Expert consensus on blood pressure management in pregnancy-induced hypertension diseases (2019). Chinese Journal of Cardiology, 48(3).
2. Zhang L, Sun L, Wei T. Correlation between MTHFR gene polymorphism and homocysteine levels for prognosis in patients with pregnancy-induced hypertension. Am J Transl Res. 2021;13(7):8253-8261
3. Yang B, Liu Y, Li Y, Fan S, Zhi X, et al. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15357 Adults of Han Nationality. PLoS ONE. 2013;8(3):e57917. doi:10.1371/journal.pone.0057917.2.
4. Kosmas, I. P., Tatsioni, A. T., & Ioannidis, J. P. A. Association of C677T polymorphism in the methylenetetrahydrofolate reductase gene with hypertension in pregnancy and pre-eclampsia: a meta-analysis. Journal of Hypertension, 2004; 22(9): 1655–1662. https://doi.org/10.1097/00004872-200409000-00004.
5. Lian Zengli, Liu Kang, Gu Jinhua, Cheng Yongzhi, et al. Biological characteristics and applications of folate and 5-methyltetrahydrofolate. Food Additives in China, Issue 2, 2022.
6. Lamers Y, Prinz-Langenohl R, Braumswig S, Pietrzik K. Red blood cell folate concentrations increase more after supplementation with [6S]-5-methyltetrahydrofolate than with folic acid in women of childbearing age. Am J Clin Nutr. 2006;84:156-161.


 Online Service
Online Service
